News
Red flags in clinical practice: expert insight on diabetic foot problems

The second article in our "Red Flags in Clinical Practice" series focuses on diabetic foot problems, in particular Charcot foot.
By Rachel Makore, Associate Clinical Negligence Solicitor
In my work as a clinical negligence solicitor, I regularly act for clients where a serious condition was not identified at the earliest opportunity.
A common feature in many of these cases is not a lack of clinical knowledge, but a failure to recognise, properly weigh, or act on key features in a patient’s presentation.
This forms part of our “Red flags in clinical practice” series, where frontline clinicians share insights into recognising time-critical conditions and understanding how delays in diagnosis can occur.
By exploring these issues from a clinical perspective, alongside the medico-legal context in which they often arise, the aim is to provide a clearer understanding of how delays in diagnosis occur and the very real consequences they can have for patients.
In this second article (you can read the first article here), Luella Robb, Diabetes Specialist Nurse shares her perspective from primary practice, focusing on diabetic foot problems and in particular Charcot foot.
Diabetic Foot Problems: The Warning Signs You Should Never Ignore
By Luella Robb, RGN, Nurse Prescriber, Diabetes Specialist Nurse
I am a registered nurse and have been working in primary care for 23 years. I specialise in long-term conditions, primarily diabetes and respiratory conditions. I qualified as a non-medical prescriber in 2013 and have been working as an advanced nurse practitioner in long-term conditions, and as a practice nurse trainer and manager, since then. I train new members of the clinical team about diabetic foot care and checks, and regularly run teaching sessions for GP registrars about the guidelines relevant to diabetic foot problems.
I have been working with Somek and Associates as a medico legal expert since 2021 and have completed several reports relating to late referral and late diagnosis of diabetic foot problems and Charcot foot.
Diabetic Foot Problems Explained
Small blood vessels and nerve endings in the feet and toes can be damaged by high levels of sugar in the blood. This leads to numbness in the feet, so that the awareness of injury is reduced, which can lead to infection and ulceration, and eventually bone destruction, gangrene and amputation. The risks of diabetic foot problems are much higher if diabetes is poorly controlled with high blood sugars.
Patients with diabetes have an annual diabetic foot check, usually at their GP surgery, where the circulation and sensation in the feet is tested. If patients are deemed to be at moderate or high risk of diabetic foot problems (because their sensation is reduced, for instance), their feet are checked more frequently.
The loss of sensation in the feet is known as peripheral neuropathy and this, along with poorly controlled diabetes and previous diabetic foot problems, significantly increases the risk of serious diabetic foot problems, including infection that gets into the bones, known as osteomyelitis and ulceration. Injuries, small cuts and blisters can all lead to severe infections and should be treated as a matter of urgency.
Charcot Arthropathy (Charcot Foot)
Charcot foot is a rare condition that can occur in diabetic patients in which bones in the foot have, unbeknown to the patient, fractured, causing tissue damage and inflammation and eventually deformity of the foot. The risks of this are increased significantly if the patient has a history of poorly controlled diabetes and/or previous diabetic foot problems. Charcot foot is a medical emergency, as it needs prompt diagnosis and treatment to prevent permanent damage.
Signs and Symptoms of Charcot Foot
- Swelling to the foot.
- Redness to the foot.
- The foot being warmer than the other foot.
- The foot looking misshapen.
- That there is often no pain.
- No recent injury.
Assessment and Advice
One of the most important markers of Charcot foot is that the affected foot is warmer than the unaffected one. The only way to assess this is to physically examine both feet. The temperature, colour and skin of both feet should be assessed, and a diabetic foot check carried out, to assess for worsening sensation or circulation.
Patients with suspected Charcot foot should be advised to immediately stop putting any weight on the affected foot, to prevent further damage being done.
Referral and Treatment
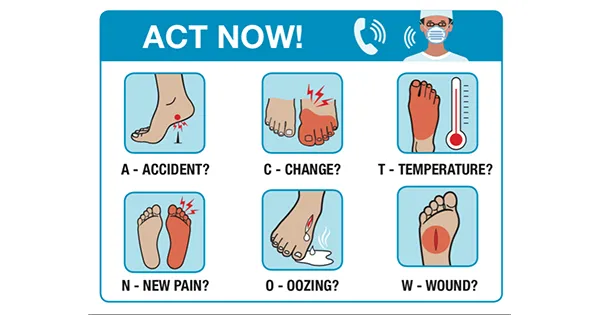
The National Institute for Health and Care Excellence guideline in diabetic foot problems states that all diabetic patients with a foot problem should be referred to their local diabetic foot clinic either on the same day as seen, or within one day. The following picture gives an indication of the problems that should result in referral.
A diagram of a person's foot
https://diabetesonthenet.com/wp-content/uploads/writing-pages-3.jpg
In the diabetic foot clinic, often called a diabetic foot multi-disciplinary team clinic, patients are assessed by specialist teams comprising of diabetes specialist nurses, diabetologists, specialist diabetic podiatrists and vascular doctors. They have access to urgent MRI scanning and specialist treatments.
Missed Diagnosis and Delayed Referral
Charcot foot is often missed in primary care because the symptoms can be mistaken for cellulitis (infection under the skin), sprains and strains, and other soft-tissue injuries.
The image below demonstrates the problem; the left foot looks red and swollen, much as cellulitis does:

The crucial thing to note is the patient’s medical history: if there is poorly controlled diabetes, previous diabetic foot problems, or poor sensation in the feet, then the likelihood of this redness and swelling being far more than simple infection or a sprain is much higher, and patients should be referred to the diabetic foot clinic as a matter of urgency.
A lack of experience in diabetic foot problems amongst clinicians can lead to misdiagnosis and late referral to diabetic foot MDT clinics; also, a lack of awareness of the NICE guideline that recommends referral to the diabetic foot MDT within one day.
Too often clinicians treat patients with antibiotics, or dressings, or opt to ‘wait and see’ what happens to a diabetic foot problem, rather than following the guidelines and referring patients into the local diabetic foot MDT immediately.
Sometimes patients are sent for X-rays of the foot, but X-rays are often unhelpful; MRI scanning is required to assess the foot for osteomyelitis and Charcot foot.
Patients can end up attending their health care providers, such as GP surgeries, with their foot problem many times over long periods of time, still putting weight on a foot that is slowly collapsing from within, before they get the investigations and treatment that they need.
Unfortunately, late referral and diagnosis for Charcot foot is fairly common, leading to delayed treatment, risking permanent deformity, loss of mobility and amputation. This leads to many legal cases against GP surgeries.
Patients who have been diagnosed with a serious diabetic foot problem continue to be cared for by the diabetic foot MDT until they have recovered. GP surgeries are often involved at this stage, if patients need frequent dressing changes to the foot. GP surgeries should also support patients to improve their blood sugar control when needed, as this will help prevent future problems. They should also have their feet checked three to six monthly and will always be regarded as having feet at high risk of diabetic foot problems in the future.
If I could change one thing…
That delays to a diabetic foot multi-disciplinary team (MDT), for any kind of diabetic foot problem, never happen.
The NICE guideline is clear, and any delay risks permanent harm to the patient, and litigation for the clinicians involved.
Contact Dean Wilson LLP
If you or a loved one has experienced a delay in the diagnosis of Charcot foot, or you have experienced other diabetic complications, and have concerns about the care received, our clinical negligence team would be happy to offer initial guidance. Please contact us on 01273 249200 or visit our Medical Negligence page for further information.
More News
On Medical Negligence

Red flags in clinical practice: expert insight on cauda equina syndrome

Sevenfold Increase In Settlement Offer In GP Negligence Claim
